
Non-surgical endodontic retreatment is often the most conservative way to save a tooth when a previous root canal did not heal the way it should, or when a tooth gets reinfected months or years later.
If you are reading this because you feel pressure when you bite, you keep getting a pimple-like bump on the gum, or your dentist mentioned a “shadow” near the root tip, you are not alone. Root canal therapy works well for many people, yet some teeth need a second pass. The good news is that modern retreatment is more predictable than it was even a decade ago, thanks to CBCT planning, microscopes, refined gutta-percha removal techniques, and stronger disinfection protocols supported by evidence-based endodontics.
This guide is written for two audiences at once: patients who want clear answers, and clinicians who want a practical, evidence-anchored roadmap. It is structured to be scannable, question-led, and easy for answer engines to quote accurately, without turning the page into a keyword dump.
What is non-surgical endodontic retreatment?
Non-surgical endodontic retreatment is a repeat root canal procedure performed through the crown of the tooth (orthograde), without surgical access through the gum. The goal is simple to describe and hard to do well: remove the old root filling, regain access to the full canal system, eliminate persistent bacteria and resistant biofilms, then seal the space so new bacteria cannot enter again.
A helpful analogy for patients: your tooth is like a house with a hidden pipe system. A first repair can be done well, yet a tiny hidden branch line can still trap debris or bacteria. Retreatment is the “open it again, clean it deeper, reseal it tighter” approach.
Why Does a Previously Treated Root Canal Fail?
Common causes of primary endodontic treatment failure tend to fall into a few buckets:
- Persistent infection
Even when a root canal is shaped and filled, bacteria can remain in fins, isthmuses, lateral canals, or apical deltas. Biofilms are organized communities, and they are harder to eliminate than free-floating bacteria. - Missed anatomy
Missed canals in molars are a classic reason for failure. Locating missed canals in maxillary molars, including second mesiobuccal canals, often requires magnification and sometimes CBCT guidance. AI-assisted detection is also entering the picture in 2026. - Coronal leakage
A crown or filling that leaks acts like an open door. Saliva bacteria can travel down microgaps, undoing even a well-cleaned root canal. - Procedural limitations or errors
Ledging, transportation, perforation, separated instruments, or an underfilled canal can leave untreated space. - Cracks or root fracture
A vertical root fracture can mimic endodontic failure. If a fracture is present, retreatment may not help because bacteria keep entering through the crack line.
Modern reviews of outcomes highlight that preoperative periapical status, lesion size, and coronal restoration quality are consistent predictors of retreatment results.

What does a persistent periapical lesion mean, and why does it matter?
When you hear “persistent apical periodontitis,” it usually means inflammation and infection around the root tip that has not resolved. On an X-ray it can appear as a dark area. On CBCT, it may look larger or more defined than on a 2D image.
Persistent apical periodontitis clinical management depends on what is driving it:
- lingering infection inside the canal system
- reinfection from a leaking restoration
- a true root fracture
- a periodontal-endodontic combined lesion
CBCT studies show that CBCT can identify periapical lesions more often than periapical radiographs, and one endodontic review reported roughly twice the odds of detecting a periapical lesion with CBCT compared with traditional imaging in outcome studies.
Why Does Non-Surgical Endodontic Retreatment Work When the First Treatment Failed?
Non-surgical endodontic retreatment works when it finds and removes the cause of reinfection, reaches anatomy that was missed the first time, and restores a tight seal from the inside and from the top of the tooth.
Several meta-analyses have reported pooled success in the mid-to-high 70% range for nonsurgical retreatment, with variation tied to case selection and outcome criteria. A 2025 clinical overview also summarizes that prior meta-analyses reported pooled success around ~76.7% to 77.8%.
A 2024 systematic review/meta-analysis reported a success estimate around 71% and noted that periapical radiolucency, lesions >5 mm, mandibular and molar teeth, and multiple-visit retreatments were linked to lower success.
What that means in plain language: many teeth do well with retreatment, but molars and large lesions are harder, and a good plan matters.
Five technical details that actually change outcomes
These are not trivia. They drive success in real cases:
- Re-establishing working length with an apex locator and radiographic confirmation, so disinfection reaches the apical system.
- Step-by-step gutta-percha removal techniques that preserve dentin and avoid pushing debris through the apex.
- Advanced irrigation protocols for root canal failures, including sodium hypochlorite delivery with activation and smear layer management (often EDTA).
- Biofilm control: disinfection of resistant biofilms in root canals requires chemistry + activation + time.
- Coronal seal: The quality of the coronal restoration is as critical as the disinfection process itself for long-term retreatment success.
How Does CBCT Technology Improve Diagnosis in Endodontic Failures?
CBCT imaging for endodontic retreatment planning gives a 3D map. It can help a clinician:
- identify missed canals and complex anatomy
- evaluate lesion size and proximity to anatomical structures
- identify resorption patterns
- support decision-making between retreatment and apical surgery
- raise suspicion for fracture patterns in certain cases
Again, CBCT’s higher lesion detection rate is not a small difference. A review reported an odds ratio around 2.04 for CBCT detecting periapical lesions compared with periapical radiography in outcome studies.
The Role of AI in 2026 Endodontics (Diagnosis, Planning, and Safety)
AI is not replacing endodontists. It is becoming a second set of trained eyes that supports consistency.
In 2026, AI-driven tools are increasingly used to assist with:
- CBCT scan review for missed canals and subtle patterns
- detection support for micro-fracture risk or vertical root fracture patterns
- automated identification of root and canal anatomy (including MB2 and complex canal configurations)
- structured reporting and triage support
A 2025 review outlines expanding AI applications in endodontics, including imaging analysis and treatment planning.
A 2026 systematic review discusses AI use in diagnosing vertical root fracture across imaging modalities, including CBCT-based approaches.
An AAE educational resource also notes that AI tools trained to detect periapical lesions in radiographs and CBCT may improve accuracy compared with unaided interpretation in some settings.
For patients, the practical benefit is simpler: fewer missed details, clearer planning, and better explanations of why a tooth needs retreatment (or why it should not be retreated).
Non-Surgical Endodontic Retreatment: Step-by-Step (What You Will Actually Experience)
Non-surgical endodontic retreatment follows a consistent clinical sequence, even though each tooth has its own anatomy and history.
Step 1: Clinical exam and diagnosis
Your dentist reviews symptoms, checks your bite, inspects the restoration margins, and evaluates gum health. X-rays are taken, and CBCT is used in many retreatment cases to guide the plan.
Step 2: Comfort plan and anesthesia
Patient comfort and local anesthesia in retreatment matter because fear is common. With proper anesthesia, you should feel pressure and vibration, not sharp pain. The team should also control dryness and visibility using a rubber dam.
Step 3: Access and isolation
The tooth is isolated to prevent saliva bacteria from entering the canal during treatment. If you have a crown, the clinician evaluates whether to go through the crown or remove it, based on structural and leakage concerns.
Step 4: Removal of old filling materials
This is where step-by-step gutta-percha removal techniques become central. Clinicians commonly combine:
- rotary retreatment instruments
- hand files for fine control
- heat-softening when appropriate
- controlled solvent use when needed
- ultrasonic support for stubborn segments
Solvents still matter in selected cases, and studies continue to compare solvent effects and performance. A 2015 study found chloroform, eucalyptol, and orange oil did not decrease dentin microhardness in that experimental setup.
A 2024 study examined orange oil solvent properties on gutta-percha and GuttaFlow-type materials.
Step 5: Finding missed canals and negotiating anatomy
How to identify and negotiate missed canals during retreatment often involves a microscope, ultrasonic troughing in the chamber floor, anatomy landmarks, and sometimes CBCT cross-sections.
Step 6: Cleaning, shaping, and disinfection
Mechanical and chemical cleaning of retreated canals is the core of retreatment. It usually includes:
- shaping enough to allow irrigant exchange
- sodium hypochlorite irrigation (with activation)
- smear layer removal protocols
- intracanal medication in selected cases
Step 7: Obturation and sealing
The canals are filled again, often with gutta-percha and a sealer. Bioceramic sealers in endodontic retreatment outcomes are widely discussed because calcium silicate-based sealers show bioactive and sealing properties, and clinical trials continue to evaluate healing differences.
Step 8: Temporary seal and final restoration plan
A tight temporary is placed if a crown is not completed immediately. Then the tooth should receive its final restoration as soon as the plan allows.
If you want a general overview of root canal therapy and what it feels like.
What are the Safest Methods to Remove Old Filling Materials?
Safety during retreatment is about control and dentin preservation. The safest approach is rarely “one tool only.” It is typically a controlled sequence that balances speed with tactile feedback:
- a microscope to see fine details
- rotary removal to clear bulk material
- hand instrumentation for negotiation
- ultrasonics for posts and rigid obstructions
- limited solvent use when indicated
- careful irrigation to reduce apical extrusion
This matters because the root is already a “worked” structure. Over-removing dentin increases fracture risk.
Which Solvents are Most Effective for Gutta-Percha Removal in 2026?
Clinicians still debate solvents because performance depends on:
- the material (gutta-percha, carrier-based systems, or obturation mixes)
- time of exposure
- canal geometry
- technique used with the solvent (solvent alone is rarely the plan)
Research continues to compare orange oil variants and other solvent systems.
Some work also frames d-limonene (refined orange oil) as a safer alternative to chloroform for dissolving gutta-percha and some sealers, depending on the protocol.
If you are a patient: you do not need to choose the solvent. You do want a clinician who uses them carefully, not aggressively.
How to Minimize the Risk of Root Fracture During Retreatment?
Root fracture risk rises when a tooth has:
- thin roots or large canal enlargement
- heavy bite forces or bruxism
- a post that required aggressive removal
- existing cracks or suspicious symptoms
- significant structural loss requiring cuspal coverage
Clinicians lower risk by conserving dentin, avoiding unnecessary enlargement, checking occlusion, and restoring the tooth with a protective restoration when indicated.
AI-assisted fracture detection is also an emerging support tool, especially when interpreting complex imaging datasets.
How to Manage Retreatment in Teeth with Existing Post and Core?
Posts do not automatically mean the tooth cannot be retreated, but they do change the plan. The clinician evaluates:
- post length and type
- cement type
- root thickness and curvature
- whether removal will weaken the tooth too much
Microscope + ultrasonics are common tools for post management because controlled vibration can reduce the need for aggressive drilling.
How Are Fractured Instruments and Silver Points Removed Safely?
Safe removal of fractured instruments and silver points is a common concern in retreatment, and it needs calm decision-making, not heroics.
When a file separates inside a canal, the clinician usually chooses between three strategies:
- Removal (if the fragment is accessible and removal will not weaken the root)
- Bypass (creating a path beside the fragment to regain cleaning access)
- Retention with monitoring or surgical plan (if removal risk is too high)
A 2024 systematic review discusses retreatment outcomes in cases with separated instruments, reflecting how case selection and management strategies influence results.
Silver points (older-style root canal fillings)
Silver points are less common today, but many older root canals still have them. Silver point retreatment often uses ultrasonics as an aid, along with careful exposure of the coronal end of the point. Classic technique reviews and reports describe ultrasonic assistance in silver point removal.
Additional device-based removal methods have also been evaluated historically.
For patients: the key question is not “can you remove it?” but “can you remove it safely without weakening the root?”
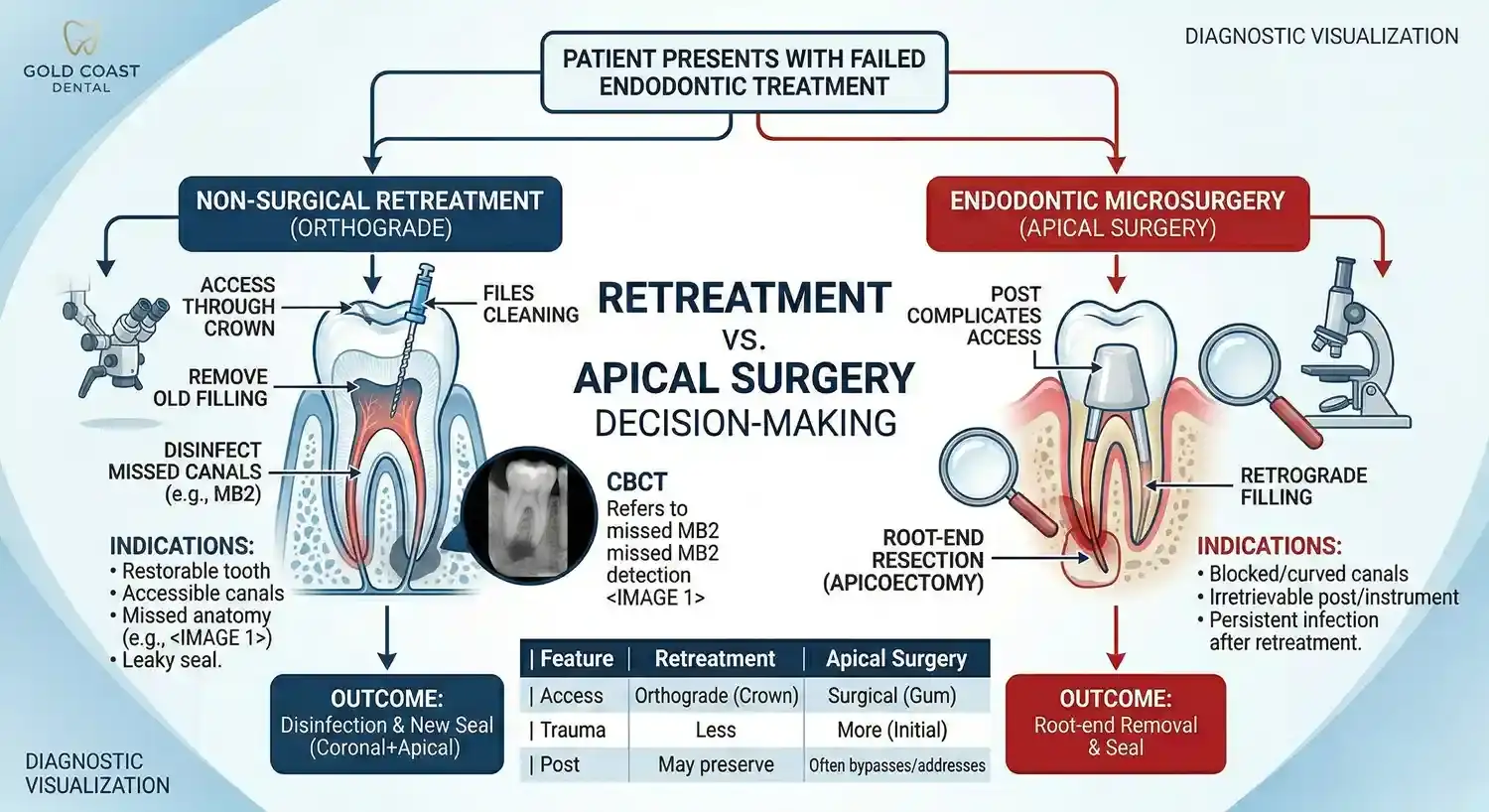
Endodontic Retreatment vs. Apical Surgery Decision-Making
Non-surgical endodontic retreatment is often preferred first when the canal system can be accessed and the tooth is restorable, because it addresses infection from inside the tooth and supports a strong coronal seal afterward.
That said, apical microsurgery can be highly successful in the right case, especially with modern microsurgical techniques and proper case selection.

Table: Comparing options (numbers vary by criteria and follow-up)
| Option | What it targets | Typical outcome signals in studies | When it tends to fit |
|---|---|---|---|
| Non-surgical retreatment | Re-cleans and reseals the canal system | Reviews summarize pooled success often around ~76–78%; a 2024 meta-analysis reported ~71% with certain risk factors lowering success | Restorable tooth, accessible canals, likely reinfection |
| Endodontic microsurgery (apical surgery) | Treats root tip infection directly with surgical access | A 2020 meta-analysis reported pooled success ~91.3% in RCTs; prospective studies show lower pooled success (~78.4%) over longer follow-up ranges | Obstruction prevents orthograde access, persistent lesion after good retreatment |
| Extraction + implant | Removes tooth and replaces it | A 2019 meta-analysis reported 10-year implant survival ~96.4% at implant level | Non-restorable tooth, root fracture, severe structural compromise |
Sources for the outcome signals above:
- Nonsurgical retreatment pooled ranges summarized in a 2025 overview and earlier meta-analyses.
- 2024 nonsurgical retreatment meta-analysis reporting ~71% success with predictors of lower success.
- Endodontic microsurgery long-term meta-analysis pooled success estimates.
- 10-year implant survival meta-analysis estimate.
A critical nuance for patients: implant survival is not the same as “no complications,” and tooth survival is not identical to “perfect radiographic healing.” You and your clinician choose based on your tooth’s structure, gum support, bite forces, and your goals.
When is it Time to Move from Retreatment to Apicoectomy?
A clinician may shift toward apical surgery when:
- the canal cannot be safely accessed (blocked canal, immovable obstruction)
- the tooth has a persistent lesion after a well-executed retreatment
- anatomy or restorations make orthograde retreatment too destructive
- the lesion pattern suggests a root-end problem that orthograde access cannot reach
Modern consensus discussions often frame apical microsurgery as minimally invasive with strong success in selected cases, especially with microsurgical protocols.
Can Bioceramic Sealers Support Better Healing in Retreatment?
Bioceramic sealers in endodontic retreatment outcomes remain a high-interest topic because calcium silicate-based sealers may support sealing and biocompatibility, and clinical studies keep testing whether this translates into better healing.
Recent randomized clinical work has evaluated lesion healing outcomes with bioceramic-based sealers and follow-up.
For patients: the sealer matters, but it does not replace the big three: diagnosis, disinfection, and restoration integrity.
What is the Gold Standard for Final Restoration After Retreatment?
Coronal restoration of endodontically retreated teeth is one of the strongest practical drivers of long-term stability. This is where many “successful” root canals fail later, not because the canals were not cleaned, but because the crown margin leaked or decay reappeared.
Evidence reviews comparing coronal restoration quality and endodontic quality show that both contribute to healing odds, and coronal seal has a meaningful role in long-term outcomes.
Newer observational work also continues to evaluate how restoration types relate to survival.
In practical terms:
- posterior teeth with significant structure loss often need cuspal coverage (crown/onlay)
- marginal integrity matters more than cosmetic perfection
- delaying the definitive restoration too long increases reinfection risk
Preparation tips (before your appointment)
These are simple, patient-centered steps that reduce friction:
- Eat a light meal unless your dentist gives different instructions.
- Take your usual medications unless told otherwise by your physician or dentist.
- Tell the team if you have anxiety so they can plan pacing, breaks, or adjuncts.
- If you have swelling, fever, or facial spread, call before arriving, as the plan may shift.
To book directly with Gold Coast Dental, If you prefer calling +15622421411
Aftercare tips (first 7 days)
Most patients do well with retreatment recovery. The main goals are pain control, bite control, and watching for unusual swelling.
What is normal
- mild soreness to chewing pressure for a few days
- mild sensitivity around the tooth
- slight gum irritation near the rubber dam area
What is not normal (call promptly)
- swelling that increases
- fever
- pain that escalates sharply after initial improvement
- difficulty swallowing or breathing
Evidence-supported pain control (common approach)
A 2022 overview of post-operative endodontic pain management reported that ibuprofen 600 mg alone and ibuprofen 600 mg combined with acetaminophen 1000 mg can be more effective than some alternatives for early post-treatment pain control in certain contexts.
Medication choice depends on your medical history, allergies, and clinician guidance, so this is not a prescription, it is the evidence context.

Evidence-based endodontics for general practitioners (a practical checklist)
Evidence-based endodontics for general practitioners is not about chasing fancy tools. It is about reducing avoidable misses and making decisions that protect tooth structure.
A clinician-facing checklist that aligns with the literature:
- Confirm restorability early (crack risk, ferrule, periodontal support).
- Use CBCT selectively for complex retreatment planning and lesion assessment.
- Use magnification when available to locate missed anatomy and manage procedural challenges.
- Prioritize irrigation activation strategies to address resistant biofilms.
- Treat coronal seal as a primary outcome driver, not an afterthought.
- When a separated instrument is present, choose removal vs bypass vs surgical plan based on dentin preservation, not ego.
- Document outcome criteria and follow-up timing clearly because “success” varies by definition and follow-up duration across studies.
Closing and next step
If you have been told you might need retreatment, non-surgical endodontic retreatment can be a strong tooth-preserving option when the tooth is restorable and the infection source is reachable. The right plan is built on careful diagnosis, modern disinfection protocols, and a restoration that seals the tooth properly.
If you want to schedule an evaluation with Gold Coast Dental, start here:
and book directly at or call +15622421411.






